IgE Food Allergy
Pathology: Food-specific IgE antibodies attach to mast cells. Mast cells are like tiny balloons filled with inflammatory chemicals. If the IgE antibodies and food allergen comes in contact, the mast cells leak their inflammatory chemicals into the surrounding tissue.
Typical IgE food allergy symptoms include:
Severe symptoms (anaphylaxis) can include a sudden drop in blood pressure (shock) and severe asthma.
Food-Symptom Interval: Symptoms usually occur within minutes to a few hours after eating.
Diagnosis: The connection between the food and symptoms is usually evident because of the short interval and consistent symptoms (occurs every time the food is eaten, even in small amounts). The diagnosis is generally based on the client’s reported symptoms and blood or skin tests confirming sensitization to the specific food.
Treatment: The food allergen is entirely responsible for the symptoms. The patient will not have symptoms if they avoid the allergen.
The immune system produces five antibody types to protect against bacteria, viruses, cancer cells, etc. Antibodies are specific (e.g., directed against a particular virus or bacteria strain). Everyone has different antibodies, depending on their exposure.
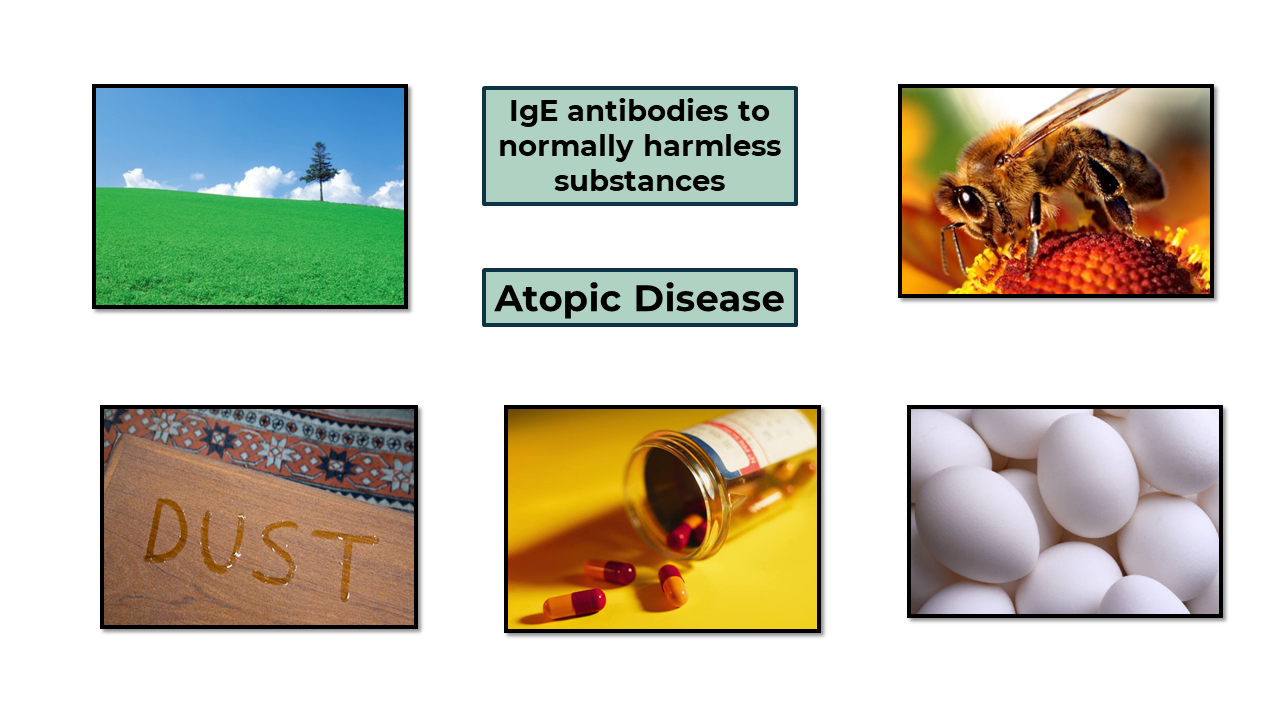
The evolutionary purpose of IgE antibodies was protection against parasitic worms. Since we no longer encounter them in our modern, clean environment, our immune system has started producing IgE to harmless compounds.
The term sensitized means the person has produced IgE antibodies. For example, “Mary has been sensitized to milk” means Mary’s immune system produces IgE antibodies directed against a milk protein.
IgE antibodies attach to mast cells and become a receptor for the allergenic protein.
Atopic disease is the genetic tendency to produce IgE antibodies to harmless compounds.
Atopy can manifest as different conditions throughout the patient’s lifetime and is often called the Atopic March.
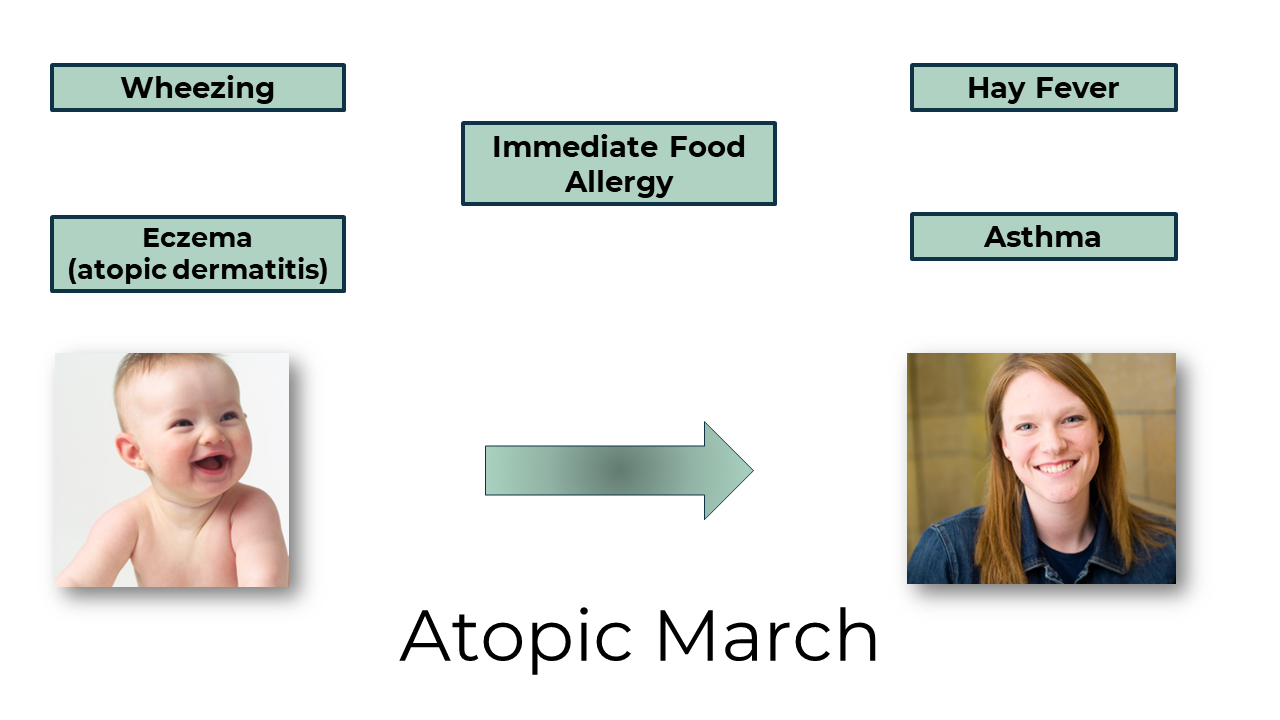
The most common symptoms during infancy are eczema (atopic dermatitis) and wheezing. These conditions often resolve, and respiratory symptoms develop (asthma and hay fever) in the late teenage and adult years. Atopic dermatitis increases the infant’s risk of developing a food allergy. Allergenic proteins come in contact with a baby’s skin (e.g., from a caregiver’s hands). If the skin is inflamed (e.g., atopic dermatitis), the protein can penetrate the skin, and the immune system reacts by producing IgE (the baby becomes sensitized through skin exposure). With an intact skin barrier, the infant’s first exposure is through the digestive tract, and tolerance usually develops.
When the IgE receptors come in contact with their allergen, the mast cells activate which releases their inflammatory chemicals into local tissue.
Symptoms depend on the following:
Typical symptoms include:
Other points to keep in mind about IgE-mediated food allergy symptoms are:
Each country has a priority allergen list based on the most problematic foods in their country. Health Canada develops the Canadian list in consultation with the medical community. Food manufacturers must declare priority allergens on their labels, even if the allergen is an ingredient of another ingredient.
The Canadian priority allergen list includes foods responsible for approximately 90% of IgE-mediated allergies and consists of the following:
Other foods can cause IgE-mediated allergy, but the incidence is less common.
The gold standard, a positive oral challenge, is impractical for routine clinic use. Therefore, physicians utilize laboratory tests.
The diagnosis starts with the patient reporting symptoms that suggest IgE-mediated allergy. The next step is determining if the patient has been sensitized to the suspected food.
Physicians use two tools:
Skin Testing
A drop of the suspected food is placed on the patient’s skin, and the physician pricks the skin (so the skin mast cells are exposed to the food). If the patient has been sensitized to the food, the mast cells release inflammatory chemicals, and a wheal (small, raised bump) will form.
Food-specific Serum IgE
The patient’s blood is tested for IgE to the suspected food.
Even though skin and blood tests have the same purpose, they often give different results (i.e., a positive blood test but a negative skin test). These tests sound simple, but they are not diagnostic and must be interpreted (in conjunction with the patient’s history) by a qualified physician.
They have a high rate of false positives because:
Sensitized ≠ Allergy
Luckily, skin and blood tests have a low rate of false negatives. For example, Sally had hives and flushing at a seafood dinner and thought she might be allergic to shrimp. Her blood test for shrimp-IgE was negative, so an IgE-mediated shrimp allergy was unlikely.
Physicians may conduct an oral challenge if the laboratory results are inconclusive.
Food-Specific IgE Blood Testing Technology
I will provide further details about the blood tests because HCPs often get questions from clients.
Almost all conventional laboratories in Canada and the United States use ImmunoCAP®. If a blood sample were sent to five labs, the results would be consistent.
Many labs also do component-resolved diagnostics. As discussed in Food Components (Module #2: Physiology Overview), IgE is directed against a specific protein within the food. A standard peanut-IgE test would indicate whether the patient is sensitized to any peanut protein. Component-resolved diagnostics would show which protein. This information can help physicians give more accurate patient recommendations. For example, specific peanut proteins are associated with milder symptoms. Additionally, specific milk protein allergies are more likely to be outgrown.
RAST (Radioallergosorbent) is the brand name of outdated technology. Unfortunately, the name is still widely used.
If you suspect your client has an IgE-mediated food allergy, please encourage them to see an allergist. Allergists are highly trained specialists who have completed a pediatrics or internal medicine residency and an additional residency in clinical immunology.
Their services include: