Celiac Disease
Pathology: Gluten triggers auto-antibody production and small intestinal atrophy.
Food-Symptom Interval: The pathological changes are delayed, so the connection between gluten and symptoms is not always obvious. However, once the patient is on a gluten-free diet, they may experience immediate digestive distress when consuming gluten.
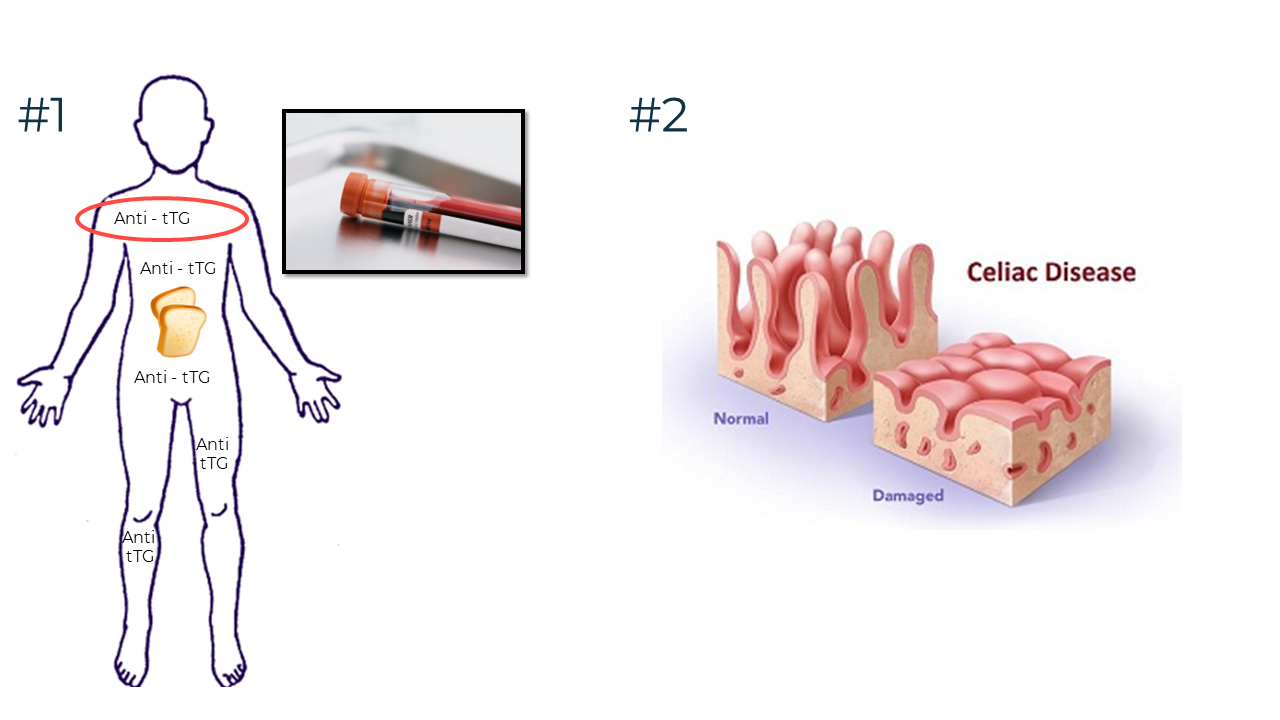
Diagnosis: If the initial screening test (auto-antibody blood test) is positive, the diagnosis is confirmed with a small intestinal biopsy (looking for atrophy).
Treatment: The only remedy is a strict, lifelong gluten-free diet.
Celiac disease is an autoimmune condition. Gluten triggers the immune system to produce auto-antibodies directed against tissue transglutaminase (tTG), an enzyme in muscle tissue. The antibodies damage the entire body and the microvilli (small intestine) atrophies. This video gives a visual representation of these concepts.
As discussed, celiac disease damages the entire body, so there is a long and diverse list of potential symptoms, including joint pain, dental enamel defects, iron deficiency anemia etc. Silent presentations (no signs) are also common.
Nutrient malabsorption also contributes to poor health and symptoms. The extent of malabsorption depends on the size and location of the atrophied patches.
Lactose intolerance is common in undiagnosed celiac disease and contributes to digestive symptoms. It usually resolves as the microvilli heal.
The diagnosis starts with a blood test to detect auto-antibodies. If the screening test is positive, the next step is a small intestinal biopsy to confirm villous atrophy. Celiac disease occursin about 1/100 of the general population, 1/20 In first-degree relatives, and 1/50 in second-degree relatives. First and second-degree relatives should be encouraged to request a screening test from their family doctor.
Diagnostic Difficulties
The diagnostic process can be complicated by:
What to Do When Patients Eliminate Gluten Before Testing
A strict, life-long gluten-free diet requires a lot of effort—particularly avoiding foods with potential cross-contamination! When clients are unsure of their diagnosis, they may not be vigilant.
If the client has eliminated gluten before being tested for celiac disease, they can:
Non-celiac gluten sensitivity is a subjective diagnosis given to clients who feel better on a gluten-free diet, but celiac disease has been ruled out. Some experts believe up to seven percent of the population is affected. However, no diagnostic markers exist to confirm who has and does not have this condition. There are many interesting theories about the potential pathology, but nothing conclusive.